





The Brazilian Butt Lift Surgery - All you need to know!
BBL Candidates - Ideal Candidates for a Butt Augmentation
Fair Amount of Fat
One of the main considerations when evaluating a patient is whether they have enough fat stored in their body. There should be enough fat available in the potential donor areas.
Patients between size 8-12, or that are slightly overweight, are usually the most qualified.
Dr. Mendieta
You have excess fat in some other part of your body to enhance your buttocks.
Dr. JenebyYou have adequate fat stores in other areas & have good skin tone in the hips and buttocks.
American Board of Cosmetic Surgery
Patients with flat buttocks and good donor fat from the back, abdomen, hips and flanks.
Dr. JungA person with intra abdominal or visceral fat is not a suited candidate. Liposuction only occurs above the muscle and below the skin.
For patients with insufficient fat deposits, the doctor may advise weight gain before the BBL to qualify for the procedure.
BMI of a BBL Candidate
The BMI, or Body Mass Index, is used by physicians as a risk indicator to assess if a potential patient could be eligible for an invasive procedure such as BBL. With BMIs greater than 30-35 the risks for complications during surgery increase. Some plastic surgeons may consider patients, with BMIs over 35, not suited for surgery. Even for some doctors a BMI of 30 is the limit.
All surgeons have their own criteria and define a patient BMI limit as to what is preferable and what is safe for a surgical intervention.
Max BMI 30
A healthy BMI is between 15-24, the maximum recommended BMI for surgery is around 30. A BMI higher than 30 is generally associated with increased surgical risks. The closer the patients are to their ideal weight the better the results. It is best to be within 10 pounds of your weight goal for at least three months prior to the BBL.
Max BMI 35
For some surgeons the max BMI for surgery is 35.
 Max BMI 30
Max BMI 30
Dr. Medina (St Domingo, D-Rep)
Dr. Schwartz (Beverly Hills, CA)
Dr. Hughes (Los Angeles, CA)
Max BMI 35
Dr. Salama (Hollywood, FL)
Dr. Tsai (West Hollywood, CA)
Dr. Potparic (Ft Lauderdale, FL)
Higher BMIs
For patients of higher BMI, their option is to lose natural weight to reach the BMI requirements.
If a patient plans to lose weight to reach an acceptable BMI (30) for the procedure, doctors recommend a slow paced weight loss accompanied with lifestyle changes to keep their new target weight.
Various surgeons recommend their patients to keep their weight for at least 6 months prior to the surgery. The idea is to maintain that weight stability even after the surgery. After the surgery, if patients lose weight the fat injected in the buttocks also shrinks.
Minimum BMI
There is no minimum BMI for any procedure. It is more a question of how much and where your excess fat deposits are located. If the patient has not much fat available, a Brazilian Butt Fat Transfer might not be the procedure to augment the size of their bottom. For thin patients unsatisfied with their buttocks butt implant surgery might be an alternative.
Explaining the Fat Transfer Procedure
Preparing the Patient
General or Local Anesthesia
This has become a debatable subject. Many surgeons have been performing BBL surgery under general anesthesia. General Anesthesia has been the general rule for BBL procedures.
The use of local anesthesia in Buttocks Fat Transfer has been more recent, and there is an increasing number of surgeons advocating for its use. Various doctors report performing liposuction using only local anesthesia without any complications for their patients. While local sedation can be common practice for small volume liposuction procedures, local anesthesia in a large Brazilian Butt Lift procedure can be very uncomfortable for the patient (Dr. Kenneth Hughes - Los Angeles, CA)
 General Anesthesia
General Anesthesia
Large volume BBL is recomended to be performed under general anesthesia.
 Local Anesthesia
Local Anesthesia
Small-volume liposuction / BBL cases can be performed with local anesthesia.
A decisive factor can be the size of the patient and the complexity of the procedure: for instance, the amount of fat to be extracted and how deep into the tissues needs the doctor to intervene.
Large Volume BBL - General Anesthesia
To get access to those deep levels of fat and tissues, and to be able to get the maximum results, surgeons opt to use general anesthesia during a BBL procedure.
Mild BBL - Local Anesthesia
Small-volume liposuction cases can be performed with local anesthesia, with or without mild sedation. However, for a combined and large volume procedure such as a BBL general anesthesia is preferred [1].
It is up to the physician and anesthesiologist to decide which type of anesthesia to use. The main goal should be patient safety.
Fat Harvesting Techniques
Specialists agree that the less traumatic the liposuction method, the higher yield of viable fat cells. This means that not every liposuction technique is adequate for a fat transfer.
Some liposuction techniques target fat cells and make them easier to extract by disrupting their structure (Laser Liposuction such as SmartLipo or Ultrasound Assisted Liposuction), while these techniques are widely popular for slimming contours, they are not suited for fat transfers.
 Tumescent Liposuction
Tumescent Liposuction
Minimally invasive harvesting methods, such as tumescent liposuction - help maintain fat cell integrity.
 Laser Assisted Liposuction
Laser Assisted Liposuction
Fat melting techniques such as (SmartLipo) can damage the fat cells, making them not suitable for re-injection.
Smart lipo uses a laser to melt and destroy fat cells. The fat cells are so damaged that they should not be used to transfer to the buttocks because the cells will not survive the transfer. Tumescent traditional liposuction is almost always used with a Brazilian Butt Lift because this technique does not laser or heat up and melt the fat cells. The fat cells are not damaged by traditional liposuction and the "take" of the fat cell is much better.
Wet or Super Wet Tumescent Liposuction is standard way of harvesting fat from the patient’s donor areas.
Preparing the treatment areas with Tumescent Solution
The tumescent method has emerged as the gold standard method in liposuction. Before liposuction begins the treatment areas of the patient are injected with a special numbing solution. This tumescent solution is a dilute that is composed of large amounts of saline mixed with a small concentration of lidocaine and even much smaller portion of epinephrine [2].
There is no official or standard formula for the tumescent solution. The levels of lidocaine and epinephrine depend on the areas to be treated and the clinical situation. The epinephrine part in the solution induces vasoconstriction allowing liposuction to be done with virtually no blood loss [3].
The solution is injected into the subcutaneous fat, so that it becomes ‘tumescent’ i.e.. swollen and firm, making it easier to remove by suction with the cannulas. It is administered warm and not cold and after 20 to 30 minutes the injected area is ready for liposuction.
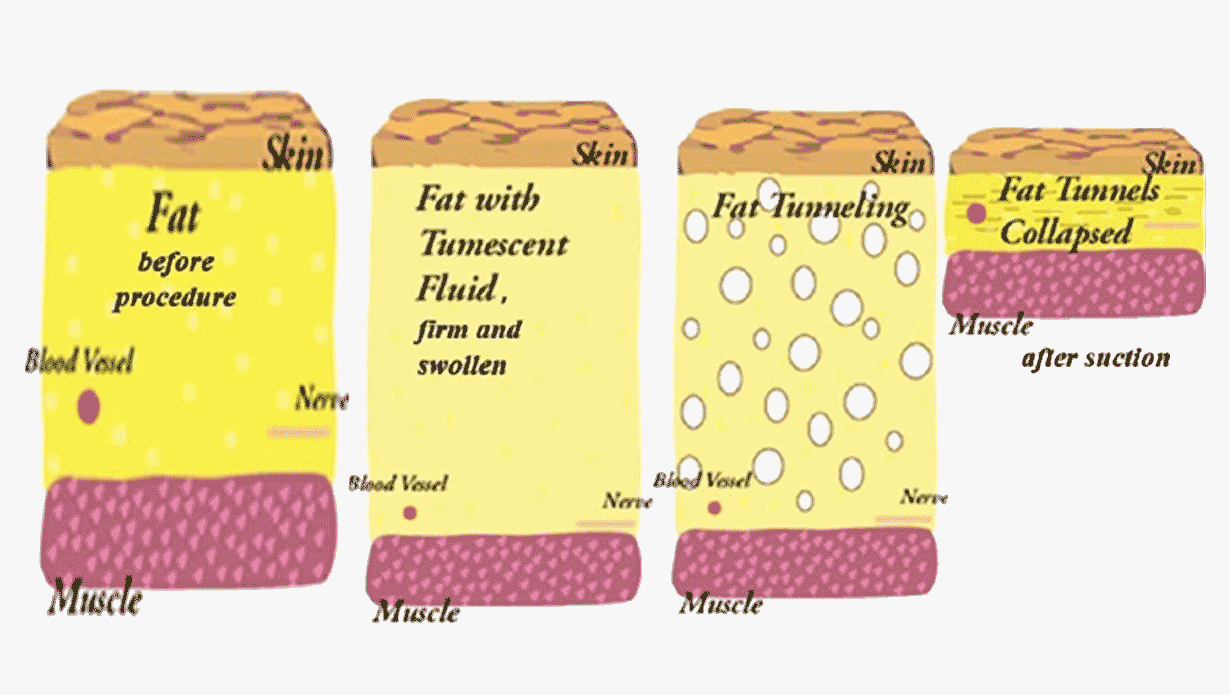 Image 1: Fat (adipose tissue) - (1) before procedure, (2) after injecting the tumescent fluid (3) after creating tunnels with the cannula (4) results after liposuction Source: Venkataram J. Tumescent liposuction: a review. J Cutan Aesthet Surg. 2008
Image 1: Fat (adipose tissue) - (1) before procedure, (2) after injecting the tumescent fluid (3) after creating tunnels with the cannula (4) results after liposuction Source: Venkataram J. Tumescent liposuction: a review. J Cutan Aesthet Surg. 2008
Points of Incision
The usual points of incision for liposuction are shown in image 2. These are standard points that allow doctors to access all fat deposits in the donor areas while keeping scars as concealed as possible.
The size of the incision should be large enough to allow the largest cannula to be used. During the procedure the surgeon might use cannulas of different diameter. The doctor will try to maintain the incisions as small as possible and place them in discrete locations. Resulting scars are usually well-concealed.
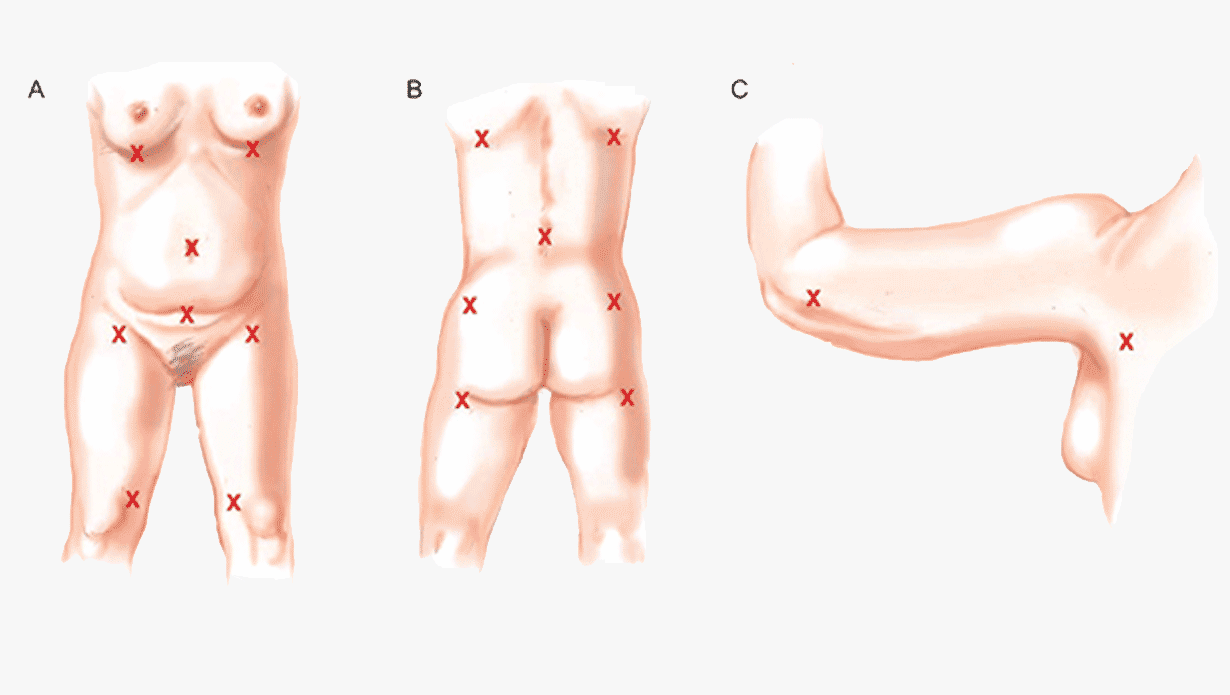 Image 2: Liposuction - common incision points. Incisions are usually placed in the bra/bathing suit line.
Source: Mendez, Bernardino M et al. “Optimizing Patient Outcomes and Safety With Liposuction.” Aesthetic Surgery Journal 39 (2019): 66–82.
Image 2: Liposuction - common incision points. Incisions are usually placed in the bra/bathing suit line.
Source: Mendez, Bernardino M et al. “Optimizing Patient Outcomes and Safety With Liposuction.” Aesthetic Surgery Journal 39 (2019): 66–82.
Positioning the Patient
Patient positioning will vary based on the location to be treated and whether any additional procedures are planned. Each position has a very specific purpose and technical goal [4].
Face up (Supine position)
Usually doctors start liposuction of the abdominal area - the patient is put in a supine position to access the front side target areas.
Lateral (Decubitus position)
The patient is then rolled to one of the two lateral positions, this makes it easier to access the fat stores of the flanks, back, arms and legs. During part of the fat reinjection - some doctors use the lateral position. This position is the best for waistline contouring.
Face down (Prone position)
This position is preferred to contour the V zone and to reshape the posterior flank area. This is also the ideal position to control buttocks symmetry.
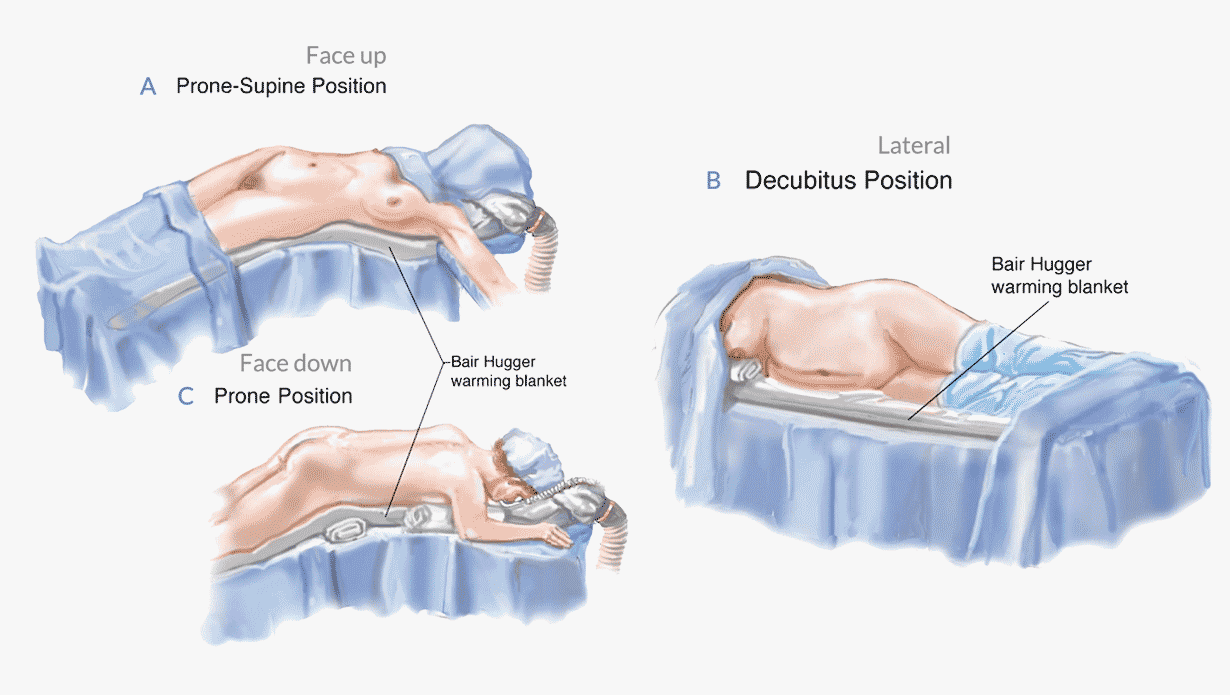 Image 3: Different positions of the patient during a BBL - (A) Prone "Face Up" (B) Decubitus "On one side" (C) Prone "Face down".
Source: Mendez, Bernardino M et al. “Optimizing Patient Outcomes and Safety With Liposuction.” Aesthetic Surgery Journal 39 (2019): 66–82.
Image 3: Different positions of the patient during a BBL - (A) Prone "Face Up" (B) Decubitus "On one side" (C) Prone "Face down".
Source: Mendez, Bernardino M et al. “Optimizing Patient Outcomes and Safety With Liposuction.” Aesthetic Surgery Journal 39 (2019): 66–82.
Liposuction - Harvesting the Fat
The fat harvesting - liposuction procedure - starts when the surgeon uses the cannula to capture the first fat deposits from the previously marked donor areas (image 4 - green colored areas).
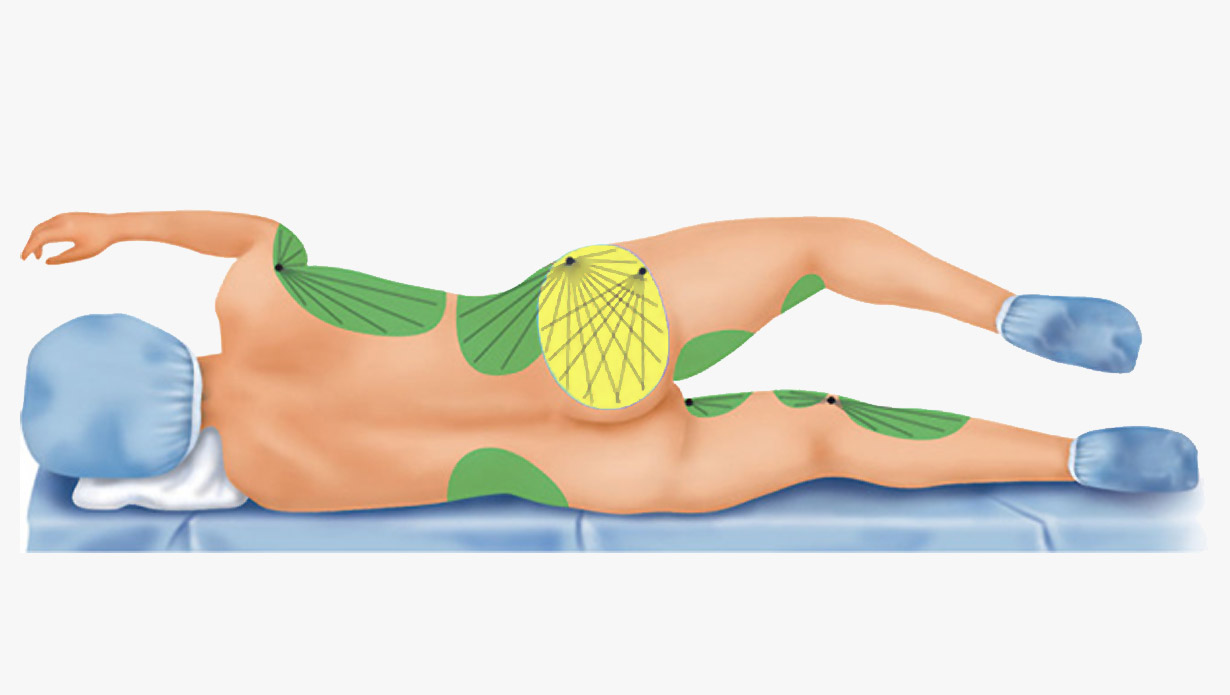 Image 4: Fat is harvested from the (green) donor areas, then placed in the buttocks (yellow).
Source: Mendez, Bernardino M et al. “Optimizing Patient Outcomes and Safety With Liposuction.” Aesthetic Surgery Journal 39 (2019): 66–82.
Image 4: Fat is harvested from the (green) donor areas, then placed in the buttocks (yellow).
Source: Mendez, Bernardino M et al. “Optimizing Patient Outcomes and Safety With Liposuction.” Aesthetic Surgery Journal 39 (2019): 66–82.
The doctor inserts the cannula in one of the incision points, then proceeds to shift the cannula back and forth carving out tunnels in the fat (this is also known as tunneling). The harvesting or tunneling is repeated on all incision points. A single area can be addressed from multiple incision points. This cross-hatched tunneling from more than 2 incision points allows to smooth out irregularities and achieve better results (see image 5).
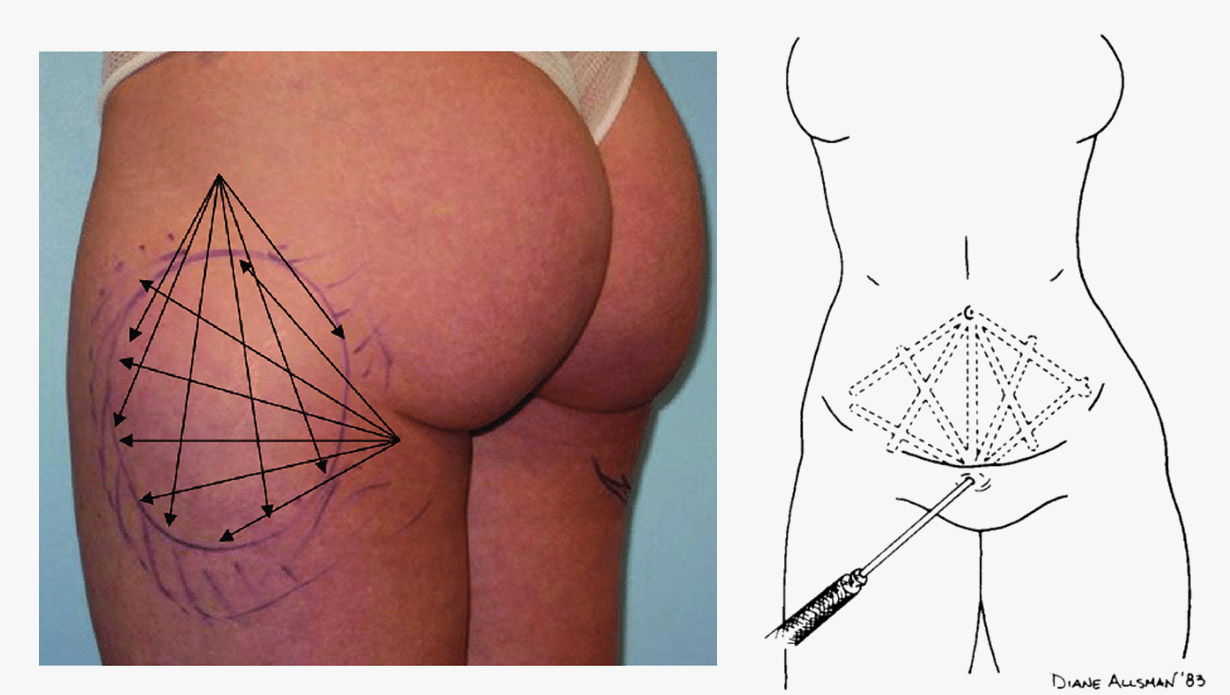 Image 5: (left) potential crosshatch of two incision points - markings (right) conventional cross hatch tunneling in abdominal liposuction Source: (left) Mordon, Serge & Plot, Eric. (2009). Laser lipolysis versus traditional liposuction for fat removal. Expert review of medical devices - (right) Newman, J., Burgermeister et al. (1991). Closed Lipo-Sweep Abdominal Liposuction. The American Journal of Cosmetic Surgery
Image 5: (left) potential crosshatch of two incision points - markings (right) conventional cross hatch tunneling in abdominal liposuction Source: (left) Mordon, Serge & Plot, Eric. (2009). Laser lipolysis versus traditional liposuction for fat removal. Expert review of medical devices - (right) Newman, J., Burgermeister et al. (1991). Closed Lipo-Sweep Abdominal Liposuction. The American Journal of Cosmetic Surgery
Cannulas come in different diameters, ranging usually between 2 mm to 5 mm.
With thicker cannulas more fat can be extracted with less effort as with a smaller cannula, but thicker cannulas also don’t produce the finer contouring results that can be achieved with thinner ones. Doctors use thicker cannulas to treat the deep layers, and smooth out irregularities with thinner cannulas in the outer more superficial areas.
Lager bore (thicker) cannulas reduce the risk of rupturing and damaging the integrity of the fat cells [5].
A study on the effects of cannula size on harvested fat showed:
- Fat cell damage (adipocyte rupture) on 25% of the fat harvested with a 3 mm cannula.
- Fat cell damage to 0% of the fat harvested with a 5 mm cannula.
For example: A doctor can begin the harvesting fat in the deep layers (to get the big chunks of fat) with a 5 mm cannula and then finish to smooth out the contours using a 3mm one (to smooth out the body contouring effect).
Purification - Preparing the harvested Fat
The fluid obtained during the liposuction part is called the Lipoaspirate.
The lipoaspirate not only contains the desired fat cells, but also other liquids such as blood, tumescent fluid and ruptured fat cells that form an oily layer (see figure 6 part D).
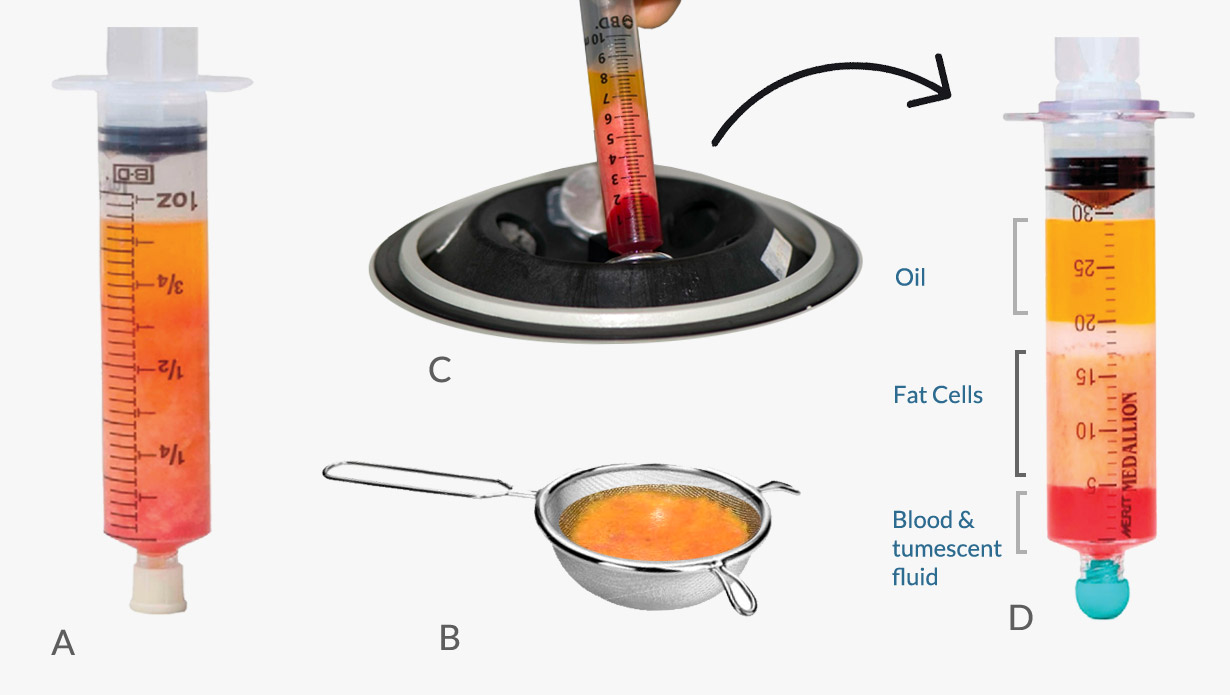 Image 6: Fat processing (A) Decantation - using simple gravity to separate the fat (B) Washing and filtration - using a steel filter (C) Centrifugation - separating particles by reinforced gravity (D) Results of separation by centrifugation
Image 6: Fat processing (A) Decantation - using simple gravity to separate the fat (B) Washing and filtration - using a steel filter (C) Centrifugation - separating particles by reinforced gravity (D) Results of separation by centrifugation
There are numerous methods to treat the lipoaspirate, to obtain only the fat cells that matter for the injection (the adipose tissue). This is known as Fat Purification or Fat Processing.
Each specialist might have their prefered fat processing method. A number of specialists advocate for washing the fat with a saline solution, while others prefer centrifugation. Some even combine methods.
There is no agreement on which is the best way to purify the fat to assure its maximum viability [6]. Also the latest medical research in fat grafting has shown that there is no single best cell-processing technique [14].
The most used fat processing techniques:
Washing with filtration
The Lipoaspirate is poured on to fine mesh stainless steel filter (similar to a steel tea filter) and soaked in a saline solution. The mix of saline solution and lipoaspirate is stirred gently with a spoon inside the steel filter [7]. Liquids such as blood, free oils and other substances such as the anesthetic fluid pass down through the filter. At the end of the washing process the filtered fat grafts are now in optimal conditions for the re-injection [8].
Decantation / Sedimentation
This method relies on separation (decantation) by gravity over a given time of the different elements present in the lipoaspirate. The Lipoaspirate is placed in syringes, which are placed vertically (plunger on the top), the aspirate is allowed to decant (sediment) for 10-15 minutes. After decantation 3 layers form in the syringe, an upper oily layer, a middle layer with fat tissue, and blood cells at the bottom [9]. Using decantation alone provides a high number of viable adipocytes, but also a good number of contaminants. Recent publications confirm that decantation shows lower graft viability compared to centrifugation and washing [10].
Centrifugation
Centrifugation is very effective in separating contaminants from the fat cells, but centrifugation at high speeds can damage part of the fat grafts [11]. For higher centrifugation speeds have a harmful effect on the viability of the processed fat grafts. Centrifugation separates the denser components from the less dense components to create layers. The upper level is the least dense and consists primarily of oil. The middle portion is primarily fatty tissue. The lowest layer is blood, water and any aqueous element. Although centrifugation can be effective in separating fat cells from other components, subjugating fat-cells to certain g-forces can damage them. Better graft viability has been reported with low centrifugal forces.
Re-injecting the Fat - Fat Grafting Techniques
The buttocks (Image 4: yellow area) are injected with the prepared fat grafts - with the patient either in a lateral or prone position (laying on her stomach). Notice the two incision points - Placing the fat graft using a fan-out and cross-hatching approach allows for enhanced contour correction.
Image 4: Fat is harvested from the (green) donor areas, then placed in the buttocks (yellow).
Source: Mendez, Bernardino M et al. “Optimizing Patient Outcomes and Safety With Liposuction.” Aesthetic Surgery Journal 39 (2019): 66–82.
When the fat graft is injected, it must be distributed evenly through the recipient site. This can be achieved by injecting it into multiple tunnels and layers. The idea is to disperse the fat in the tissue instead of allocating it in one single area.
The fat is reinjected following the withdrawal of the cannula. This means that cannula is inserted first, the doctor then starts and keeps injecting the fat as long as the cannula is withdrawn.
The surgeon leaves a fat cell path while withdrawing the cannula (image 7) [15].
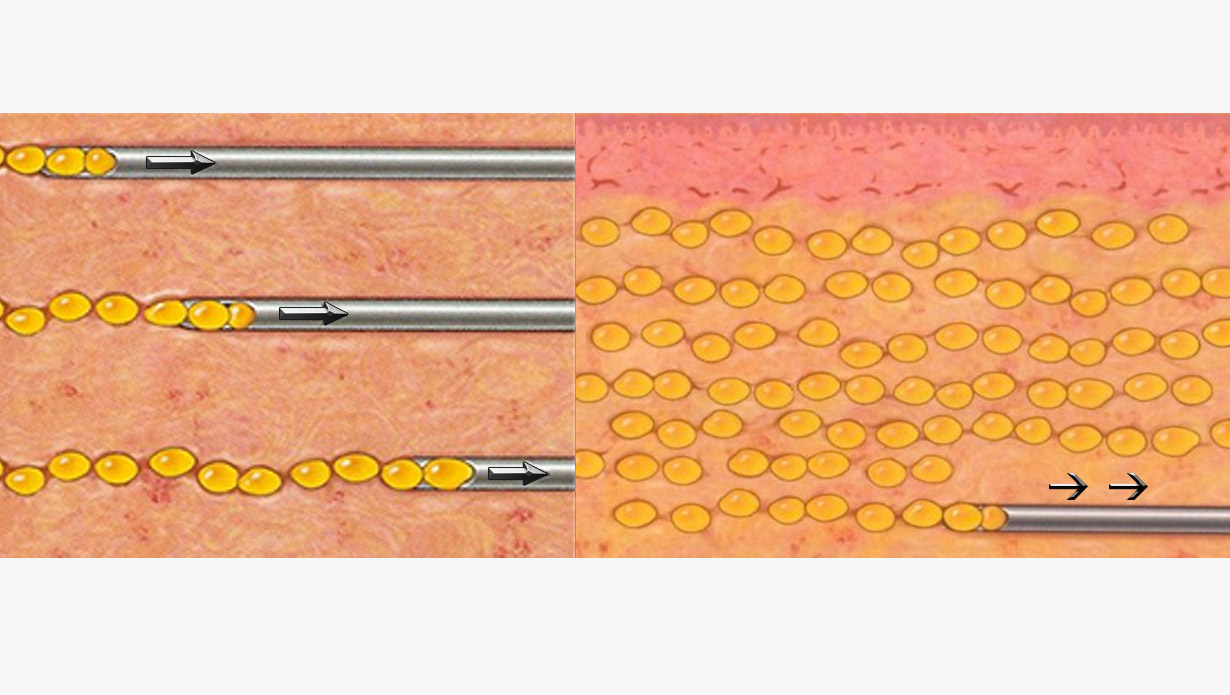 Image 7: The fat is injected by leaving small amounts of grafts with each withdrawl movement of the cannula - like sowing seeds.
Source: Levi, B. (2015). The Current State of Fat Grafting A Review of Harvesting, Processing, and Injection Techniques. Plastic & Reconstructive Surgery
Image 7: The fat is injected by leaving small amounts of grafts with each withdrawl movement of the cannula - like sowing seeds.
Source: Levi, B. (2015). The Current State of Fat Grafting A Review of Harvesting, Processing, and Injection Techniques. Plastic & Reconstructive Surgery
Shape & Volume: Reinjecting the fat has two purposes, (1) to contour/reshape to (2) add volume to the glutes [4].
Fat injected at a slow rate (low shear stress) results in better fat graft retention than fat injected at a fast rate (high shear stress) [13].
As for the fat reinjection, every doctor might follow a different technique.
Traditional Syringe Injection (Coleman technique)
Some doctors prefer a more traditional fat-reinjection approach. They manually re-inject the fat using a 60-ml syringe tipped with a cannula instead of a needle. One of the problems with the syringe is the pressure applied while injecting the grafts. Fat injected at a slow rate (low shear stress) results in better fat graft retention than fat injected at a fast rate (high shear stress). The doctor has to keep control on the pressure he uses in the syringe plunger.
Assisted Injection
Other doctors use assisted reinjection technology. Expansion Vibration Lipofilling is one example of assisted re-injection. Here the surgeon if freed from having to push the plunger of a syringe, the fat grafts are pumped through a vibrating hand device tipped with an upward bent (4 to 5 mm) cannula. According to the inventor of this technique, one of the benefits is less arm fatigue for the surgeon. Also, with an assisted system - pressure placed on the fat cells can be controlled.
Safe Gluteal Fat Injection
On January 31, 2018 the Inter-Society Gluteal Fat Grafting Task Force* released a practice advisory for gluteal fat injection procedures with the intention to define clear doctor patient safety education measures.
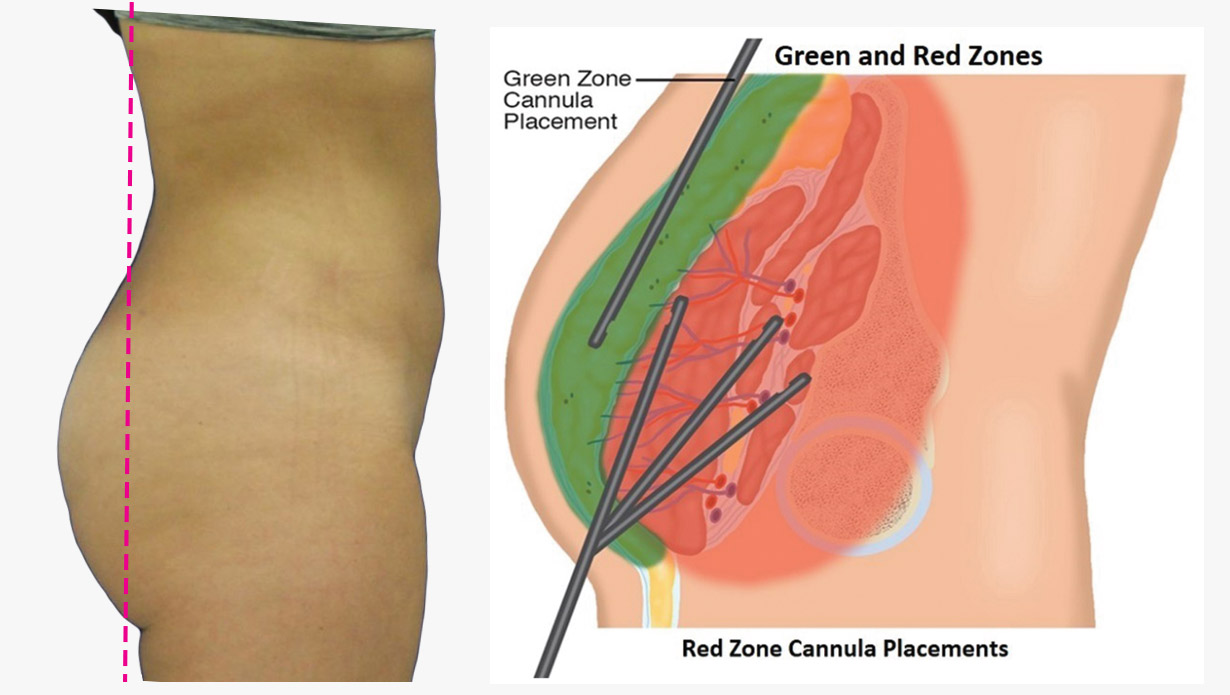 Image 8: (Green) safe zones for cannula placement during gluteal augmentation. The red zone should be avoided for the safety of the patient.
Source: Kalaaji, Amin & Dreyer et al. (2018). Gluteal Augmentation With Fat: Retrospective Safety Study and Literature Review. Aesthetic Surgery Journal.
Image 8: (Green) safe zones for cannula placement during gluteal augmentation. The red zone should be avoided for the safety of the patient.
Source: Kalaaji, Amin & Dreyer et al. (2018). Gluteal Augmentation With Fat: Retrospective Safety Study and Literature Review. Aesthetic Surgery Journal.
The Fat Injection Safety suggestions are:
- Avoid injecting fat into the deep muscle
- Avoid pointing the cannula downward, maintain a parallel angle to the patient’s back
- Keep the cannula away from the gluteal veins
- Focus all the time on the position of the cannula
- Use a 4.1 mm or thicker cannula
- Position the patient and create incisions to create safe subcutaneous injection paths
- Inject fat only with the cannula in motion - avoid high pressure big chunk (bolus) injections.
* The Inter-Society Gluteal Fat Grafting Task Force represents leading clinical plastic surgery societies, including the American Society of Plastic Surgeons (ASPS), the American Society for Aesthetic Plastic Surgery (ASAPS), and the International Society of Aesthetic Plastic Surgeons (ISAPS).
If the fat does not receive blood supply within a short period of time, it will die and can become a scar tissue, so it is really important that the plastic surgeon you choose has great experience and technique.
How much Fat can be safely transferred?
The amount of fat to transfer during a BBL procedure is determined by the doctor and varies from case to case.
There is no consensus as to what is the safest maximum amount of fat to transfer.
Being aware that there is a certain risk associated with a buttocks fat transfer - such as fat necrosis and fat embolism, researchers started to question if higher volume fat transfers could also mean a higher risk. How much volume of fat reinjection is considered safe? Should there be a limit?
According to a study published in 2018, 137 high volume butt augmentation cases were analyzed. Every patient received at least 1000 ml in each buttock [12].
No increased Risk was found -- with High Volume BBL surgeries (over 1000 ml of injected fat per buttock). As long as the fat is transferred under the skin and not in the muscle - as suggested by the Inter-Society Gluteal Fat Grafting Task Force - fatality risks can be minimized.
References
- [1] Chia, C., Theodorou, S., Dayan, E., Tabbal, G., & Del Vecchio, D. (2018). “Brazilian Butt Lift” under Local Anesthesia: A Novel Technique Addressing Safety Concerns. Plastic and Reconstructive Surgery, 142(6), 1468-1475.
- [2] COLDIRON, B., COLEMAN, W., COX, S., JACOB, C., LAWRENCE, N., KAMINER, M., & NARINS, R. (2006). ASDS GUIDELINES OF CARE FOR TUMESCENT LIPOSUCTION. Dermatologic Surgery, 32(5)
- [3] Regula, C., & Lawrence, N. (2014). Update on Liposuction: Laser-Assisted Liposuction Versus Tumescent Liposuction. Current Dermatology Reports, 3(2), 127-134.
- [4] Constantino Gilberto Mendieta, Gluteal Reshaping, Aesthetic Surgery Journal, Volume 27, Issue 6, November 2007, Pages 641–655
- [5] Cervelli, D. (2014). The Impact of Liposuction Cannula Size on Adipocyte Viability. Annals of Plastic Surgery, 73(2), 249–251-249&ndash-ndash;251-249–251.
- [6] Alexandra Condé-Green, Natale Ferreira Gontijo de Amorim, Ivo Pitanguy, Influence of decantation, washing and centrifugation on adipocyte and mesenchymal stem cell content of aspirated adipose tissue: A comparative study, Journal of Plastic, Reconstructive & Aesthetic Surgery, Volume 63, Issue 8, 2010, Pages 1375-1381
- [7] Pawitan, J., Liem, I., Suryani, D., Bustami, A., & Purwoko, R. (2013). Simple lipoaspirate washing using a coffee filter, Asian Biomedicine, 7(3), 333-338. doi: https://doi.org/10.5372/1905-7415.0703.184
- [8] Dos-Anjos Vilaboa S, Llull R, Mendel TA. Returning fat grafts to physiologic conditions using washing. Plast Reconstr Surg. 2013;132(2):323e–326e. doi:10.1097/PRS.0b013e3182958be1
- [9] Gontijo-de-Amorim NF, Charles-de-Sá L, Rigotti G. Mechanical Supplementation With the Stromal Vascular Fraction Yields Improved Volume Retention in Facial Lipotransfer: A 1-Year Comparative Study. Aesthetic Surgery Journal. 2017 Oct;37(9):975-985. DOI: 10.1093/asj/sjx115.
- [10] Cleveland, Emily & Albano, Nicholas & Hazen, Alexes. (2015). Roll, Spin, Wash, or Filter? Processing of Lipoaspirate for Autologous Fat Grafting: An Updated, Evidence-Based Review of the Literature. Plastic and reconstructive surgery. 136. 706-713
- [11] The effect of centrifugation on viability of fat grafts: an evaluation with the glucose transport test. Xie, Yun et al. Journal of Plastic, Reconstructive & Aesthetic Surgery, Volume 63, Issue 3, 482 - 487
- [12] Pane, T.A. (2019). Experience With High-Volume Buttock Fat Transfer: A Report of 137 Cases. Aesthetic Surgery Journal, 39(5)
- [13] The effect of pressure and shear on autologous fat grafting. Lee JH, Kirkham JC, McCormack MC, Nicholls AM, Randolph MA, Austen WG Jr. Plast Reconstr Surg. 2013 May;131(5):1125-36.
- [14] Wolters Kluwer Health. "Best way to prepare fat cells for grafting? Jury's still out." ScienceDaily. ScienceDaily, 28 September 2015.
- [15] Levi, B. (2015). The Current State of Fat Grafting A Review of Harvesting, Processing, and Injection Techniques. Plastic & Reconstructive Surgery, 136(4), 897–912-897&ndash-ndash;912-897–912.
- [16] Kalaaji, Amin & Dreyer, Stine & Vadseth, Line & Maric, Ivana & Jönsson, Vanja & Haukebøe, Trond. (2018). Gluteal Augmentation With Fat: Retrospective Safety Study and Literature Review. Aesthetic Surgery Journal. 39. 10.1093/asj/sjy153.
- Venkataram J. Tumescent liposuction: a review. J Cutan Aesthet Surg. 2008;1(2):49–57. doi:10.4103/0974-2077.44159
- Mendez, B.M., Coleman, J.E., & Kenkel, J.M. (2019). Optimizing Patient Outcomes and Safety With Liposuction. Aesthetic Surgery Journal, 39(1)
- Mordon, Serge & Plot, Eric. (2009). Laser lipolysis versus traditional liposuction for fat removal. Expert review of medical devices. 6. 677-88. 10.1586/erd.09.50.
- Newman, J., Burgermeister, H., & Golshahi, M. (1991). Closed Lipo-Sweep Abdominal Liposuction. The American Journal of Cosmetic Surgery, 8(1), 3-8.
- Solomon, G. (2016). Buttock Augmentation. The American Journal of Cosmetic Surgery, 33(3), 145-151.
- Whitfield, R., Rios, L., & DiBernardo, B. (2017). Making Fat Transfer to Buttocks Safer. Aesthetic Surgery Journal, 37(10), 1199-1200.
- Mills D, Rubin JP, Saltz R. Multi-society gluteal fat grafting task force issues safety advisory urging practitioners to reevaluate technique. https://www.surgery.org/sites/default/files/Gluteal-Fat-Grafting-02-06-18_0.pdf
- Roberts, T., Toledo, L., & Badin, A. (2001). Augmentation of the Buttocks by Micro Fat Grafting. Aesthetic Surgery Journal, 21(4), 311-319.
- Mendieta, C. (2007). Gluteal Reshaping. Aesthetic Surgery Journal, 27(6), 641-655.
